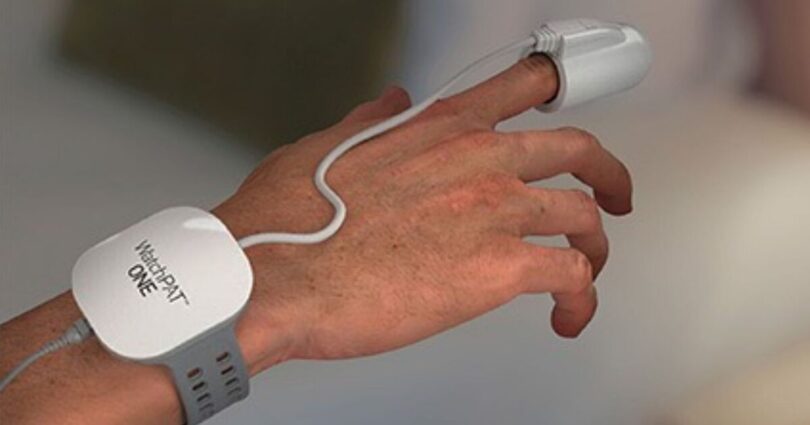
A simple WatchPat device linked to your smartphone can reveal if you have a sleep condition (Image: The Better Sleep Clinic)
Sleep disorders and poor-quality sleep are on the rise, with up to a third of Brits affected by conditions like insomnia and obstructive sleep apnoea, a condition associated with loud snoring. It can also have a serious impact on your long-term health.
With cases more than tripling in the last decade, key factors driving this increase include obesity. So what causes sleep apnoea and what can be done about it?
What is obstructive sleep apnoea?
Obstructive sleep apnoea, or OSA, is a sleep disorder usually associated with snoring where your upper airway repeatedly closes as you sleep. This leads to extremely fragmented and poor-quality sleep.
What are the symptoms?
Night-time symptoms of OSA include loud snoring, which can be disruptive to your sleeping partner, pauses in breathing, and even choking or gasping sounds. Daytime symptoms include significant daytime sleepiness, poor concentration and memory loss. One in five patients also report depression.
Why it happens
Large parts of your upper airway are made up of soft tissues held in place by muscles. As you fall asleep, these muscles relax, which leads to a natural narrowing in your airway.
With this, you can start to get turbulent airflow as you breathe, causing the tissues to vibrate, which is why we snore.
With OSA, your airway actually closes entirely and your breathing pauses – this is known as apnoea. Your body can only tolerate this for so long before it essentially sets off an alarm and pulls you back from deeper sleep to a shallower state, or you awake completely so your airway muscles regain strength, pull open your airway and you can start breathing again. Your breathing often restarts with a snorting sound.
This can make it difficult to get into a deeper state of sleep because whenever you do, your airway closes, you stop breathing, and your body has to wake you up again.
Simple sleep test left my long-suffering wife feeling smug

Express Associate Editor Matt Nixson after undergoing sleep test (Image: Phoebe Nixson)
My wife has complained for years about my snoring. And in fairness, having recently recorded my nocturnal noises and made me listen to them, she has a point. (And I now realise why she ends up on our sofa bed in the lounge quite so often.)
But is my snorting, snuffling and gasping the result of middle-aged spread and my love of beer – or a sign of something more serious? To find out, Dr David Garley set me up with a simple WatchPAT test. Having downloaded the app,I placed the strap around my wrist and slipped my left middle digit into the finger monitor. Next, I attached a sticky sensor to my chest, at the top of my breastbone, as I had been instructed.
Feeling sleepy, I pressed start on my smartphone and rolled over, ready for my experiment. Next morning, having (as far as I knew) slept soundly through the night, I unplugged myself and turned off the device – automatically sending my results to the lab to be examined. Less than 24 hours later, my wife was in full “I told you so” mode.
According to the data, it took me just two minutes to fall asleep (I’ve always thought my ability to drop off anywhere at any time was a superpower – David says it’s actually probably due to exhaustion) and slept for seven hours 49 minutes. I had five short awakenings during the night and spent 11% of my sleep in REM – when the brain rests and repairs itself best – less than half of the norm. More alarming was my AHI (apnoea-hypopnoea index) – the number of pauses in breathing per hour of sleep. Mine was 37 – hence my wife’s smugness.
“An AHI of 37 means you stop breathing 37 times every hour,” explains David. “You will struggle to get into the deep stages of sleep because whenever you do, your airway closes and you stop breathing. This causes extremely fragmented and poor quality sleep, which explains your increased sleepiness during the day.
“Interestingly, some people with sleep apnoea feel they ‘sleep well’ because they fall asleep immediately. But this often suggests a degree of sleep deprivation.”
He continues: “While anyone can get sleep apnoea, it is more common if you are carrying a bit of extra weight, and so reducing BMI can help here. However, the gold standard treatment is CPAP (continuous positive airways pressure). This treatment can very effectively control the airway blockages during sleep. It allows you to continue to breathe freely as you fall into deeper states of sleep. With this increased sleep quality, you should find yourself waking up feeling more refreshed and having more energy during the day.”
So there you have it. Watch this space!
 device")
Patient wearing a CPAP (continuous positive airway pressure) device to prevent apnoea (Image: The Better Sleep Clinic)
The impact on health and wellbeing
Think back to the last time you didn’t sleep well – how did you feel? Probably awful. Physically fatigued, unable to concentrate, memory problems and probably feeling very grumpy. And this is after one night of poor sleep.
So imagine not sleeping well for a week, or a month, a year, or even five years, and the impact on your health is much more sinister.
Habitual poor sleep is strongly associated with cardiovascular diseases such as high blood pressure, heart attacks and strokes. It significantly increases your risk of diabetes, and can also cause depression.
OSA often creeps in over months or years. Commonly in clinic, we find that people have had symptoms for well over a decade without raising the alarm and they can be in a really bad physical as well as mental state.
The other serious health risk associated with obstructive sleep apnoea happens on the road. A staggering one in five car crashes are associated with poor sleep. If you have OSA, your crash risk is four times that of drivers who have slept well and are properly rested.
Who gets OSA?
The bottom line is that anyone can get sleep apnoea. However, there are some risk factors that make the condition more likely.
The most important of these are weight and age. If you’re carrying a bit of extra weight, especially if it’s around the shoulders and neck, this can push in on the airway and make it slightly narrower.
This isn’t necessarily obesity – if you are very muscular, this can have the same effect, and this is why athletes who carry out power sports like bodybuilding or rugby often have high rates of OSA.
As you get older, the soft tissues in the upper airway become slightly lax, and this means your airway has more of a habit of narrowing in during sleep.
Men are more likely to get OSA, however, the protective effects of oestrogen women have starts to reduce in perimenopause, which is why OSA becomes a lot more common at that time.
There are other conditions that can make sleep apnoea more likely. Anything that causes swelling and inflammation of the airways such as hay fever, rhinitis or smoking. Also, anything that can make the muscles of the upper airway slightly weaker, such as alcohol and certain medications.
The really big myth is that OSA is only a condition for older people with higher BMIs. This isn’t true and a lot of sleep apnoea often relates to the shape of your airway due to anatomy.
So, regardless of your age, weight or sex, if you have symptoms, it could be OSA.

Dr David Garley of The Better Sleep Clinic warns that apnoea can be deadly if untreated (Image: The Better Sleep Clinic)
Diagnosis
There is a helpful quiz you can try called STOP-Bang. But because one of the main symptoms is daytime sleepiness, this can be assessed through a different questionnaire called the Epworth sleepiness scale.
If you are considered higher risk, the next step is a sleep test. In the old days, this was always done in a hospital when you were wired up to a big machine, but now technology has advanced, and the tests are nearly always carried out with much easier home sleep tests.
These devices are different to the kind of wearable tech devices that you might have. They take extremely detailed measurements on your sleep, including oxygen and heart rates, body position, snoring and respiratory effort, and also some more intricate measures of your nervous system and how this can respond to obstructed breathing overnight.
The main measurement that is needed is called the AHI (apnoea-hypopnoea index). This is the number of times you stop breathing per hour of sleep. Up to five times an hour is allowed. Five-15 is mild, 15-30 is moderate and above 30 is severe. We have seen patients experiencing an AHI of over 100, which means every hour they stop breathing 100 times.

A WatchPat device can diagnose conditions over a single night’s sleep, as Matt Nixson discovered (Image: The Better Sleep Clinic)
What are the treatments?
The good news is that obstructive sleep apnoea is a treatable condition. It can be helped with implementing lifestyle measures such as losing weight if appropriate, stopping smoking, or reducing alcohol intake.
Some people find that their sleep apnoea is significantly worse when they lie on their back, and so in these situations, finding a way to sleep more consistently on your side can help. This can be achieved through triangular-shaped pillows or sometimes some backpack devices which can stop you rolling on to your back.
There are dental devices too, known as mandibular advancement devices, which are like sports gum shields but with a section for the lower jaw. These clip together to bring your lower jaw forwards slightly in order to create a bit more space in the airway behind the tongue.
These tend to be better for simple snoring, or the milder forms of OSA. The gold standard treatment for obstructive sleep apnoea is called CPAP (continuous positive airway pressure). This is a small box that sits on your bedside table and blows air at a low pressure through a tube, to a mask and gently holds your airway open from the inside. This way, as you fall asleep, your airway is supported and doesn’t close in on itself.
This means that you can continue breathing as you sleep and get into those really deep states of sleep that you need to get in order to feel properly refreshed in the morning. It is always important to be set up properly with a CPAP machine and have your use followed up to make sure that you are making the expected progress and have the right support if you have any questions on how to use the treatment.
Dr David Garley is director of The Better Sleep Clinic. Visit thebettersleepclinic.co.uk for more information
Source link





